The data is in and it’s becoming increasingly clear that the impacts of commercial marijuana industry are even worse than we thought, particularly for America’s young people. A new report released by Smart Approaches to Marijuana shows the reality in "pot-legal states" paints a vastly different picture than the common sales pitch of the industry and supporters of legalization.
The marijuana industry, which spent billions to lobby elected officials and bankroll legalization referendum campaigns, is following the playbook pioneered by Big Tobacco. They recognize that the road to big profits runs through the heaviest users. As such, they have increased potency of the drug by more than four times since 1998, hoping to hook kids while they are young and vulnerable. The numbers show that it’s working.
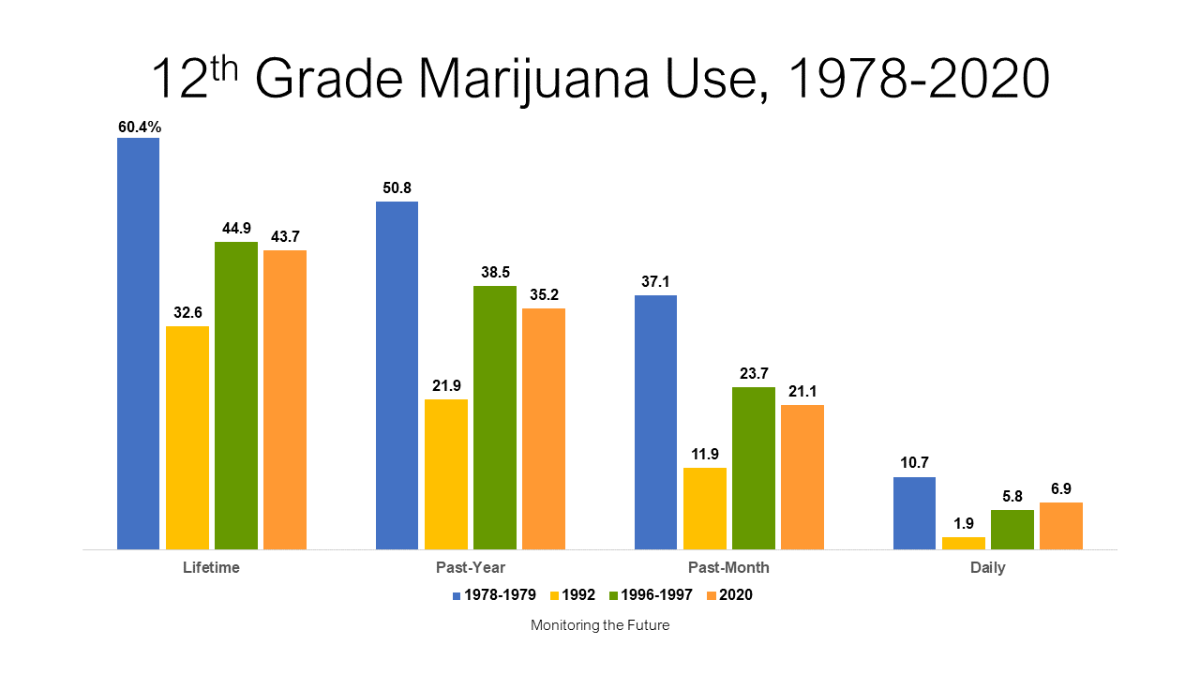
Usage rates have reached record highs among those who are most vulnerable to marijuana’s long-term health effects. The National Institute on Drug Abuse warned, "Past-year, past-month, and daily marijuana use (use on 20 or more occasions in the past 30 days) reached the highest levels ever recorded" among those aged 19 to 30. The percentage of 8th, 10th and 12th graders who used marijuana daily has more than tripled between 1991 and 2020.
Daily marijuana use is indicative of a marijuana use disorder, also known as addiction to marijuana. For all the talk about how pot is not addictive, in 2021, 1.3 million individuals between the ages of 12 and 17 had a marijuana use disorder, accounting for more than 46% of users in that age group. Legalization is also associated with a 25% increase in marijuana use disorder among them as well.

Jeremy Baldwin tags young cannabis plants at a marijuana farm operated by Greenlight, Oct. 31, 2022, in Grandview, Mo. Voters in North Dakota and Arkansas have rejected measures to legalize marijuana, while those in Maryland have approved legalization. Similar measures also were on the ballot in Missouri and South Dakota. (AP Photo/Charlie Riedel, File)
As usage rates, potency and addiction have increased, the adverse effects have also increased. Though supporters of legalization like to downplay the risks of marijuana, the drug caused more than 70,000 individuals younger than 18 to have marijuana-related emergency department visits in 2021.
The industry told parents and politicians that they would not target kids. That’s turned out to be false. From "Pot Tarts" to "Stoney Patch Kids," the packaging of edibles laced with high-potency THC often looks like traditional snacks. Not surprisingly, between 2017 and 2021, there was a 1,375% increase in at-home exposures to marijuana edibles involving children younger than 6.
More minors are driving under the influence of marijuana too. In 2021, 10.67 million people admitted to driving under the influence of marijuana, including 1.36 million who were between the ages of 16 and 20. There were 2.41 times more minors on the road under the influence of marijuana than were under the influence of alcohol.
Minors have also gravitated toward marijuana vapes, products engineered to include a near-pure form of THC. Between 2017 and 2020, the percentage of 12th graders who vaped marijuana increased from 9.5% to 22.1%. Among 10th graders, it increased from 8.1% to 19.1%, and among 8th graders, it increased from 3.0% to 8.1%. A 2022 study found, "cannabis vaping is increasing as the most popular method of cannabis delivery among adolescents in the United States." and frequent use is increasing faster than occasional use.
The marketing scheme of the industry has been to engineer a more potent drug, in forms easier to consume and while stoking the perception that it’s harmless. In 1991, 78.6% of 12th graders believed that using marijuana regularly puts one’s health at great risk. But in 2021, only 21.6% held this viewpoint. Those who hold that point of view are six times more likely to use it than individuals who perceive it as being high risk.
By 2021 nearly seven in 10 12th graders seemingly approve of marijuana use.
We all want the best future for our children. Yet, the growth of the pot industry has provided kids with greater access to a drug that medical science links to psychosis, depression, suicidality, and lower IQ at a time when the brain is still developing. Regular users are nearly five times more likely to develop a psychotic disorder and users of high-potency marijuana are four times more likely than users of low-potency products to become addicted.
More young people are becoming addicted to marijuana, and it is sending more of them to the hospital. More of them are using a more potent form of the drug. It is past time for our nation to reverse course and advance drug policies that protect our children, rather than allow them to be collateral damage for another Big Tobacco.