


If vulnerable patients are going to take powerful hallucinogens, they deserve better evidence.
Read MoreStay in the know with the latest on our fight against the legalization of marijuana
Have an article that you would like us to post? Share it on our Facebook page!
What You Aren’t Hearing About Marijuana’s Health Effects→
/
Bertha Madras, a leading expert on weed, outlines the science linking it to psychiatric disorders, permanent brain damage, and other serious harms.
Read MoreMarijuana Is More Dangerous Than Biden’s HHS Lets On→
/
In easing restrictions, it brushes past the long-term effects, from anxiety and depression to psychosis.
Read MoreAnalysis of HHS Cannabis Rescheduling Rationale
/On August 30th, 2023, the Department of Health and Human Services (HHS) announced it recommended the reclassification of marijuana to Schedule III to the Drug Enforcement Administration (DEA). Four months later, HHS released an unredacted version of its recommendation to reclassify the drug. The 252-page review had been hidden from the public and was only released after legal action was threatened against HHS.
This HHS recommendation is based on cherry-picked data and represents a weak and intellectually dishonest argument to reschedule marijuana. This summary describes just a few of the many flaws in the HHS methodology and conclusions. SAM’s full report provides an in-depth analysis of what the HHS got wrong and how the process could have been strengthened.
1. In years past, the FDA, an agency of the HHS in charge of approving medicinal drugs, used an established five-factor analysis in determining whether Schedule I drugs have “currently accepted medical use.” In the current report supporting the recommendation to reschedule marijuana, the FDA changed these criteria to get its desired answer.
If marijuana had been held to the same standards as other drugs, it would not be deemed to have “currently accepted medical use,” due to the infeasibility of measuring all strains and the insufficient amount of existing research into its safety and efficacy. In fact, the FDA’s new two-factor test explicitly states that studies used to support marijuana’s accepted medical use do not need to be controlled, a standard that was required in the five-factor test (save an evaluation done by a consensus of experts).
2. It is not clear why the FDA moved away from the five-factor test, unless the agency approached the rescheduling review with a pre-determined conclusion.
The five-factor test has been used for decades by Republican and Democratic Administrations. Additionally, the United States Court of Appeals for the District of Columbia Circuit examined and validated the test in Alliance for Cannabis Therapeutics v. Drug Enforcement Administration. The marijuana industry petitioners in that case even conceded that the five-factor test had no flaws, as explained in the opinion for the court.
3. The FDA now considers the existence of state medical marijuana programs as evidence that marijuana has currently accepted medical use.
A drug’s popularity among the public has never been used as a standard to determine medicine. Supreme Court Justice Steven Breyer in Gonzalez v Raich (545 U.S. 1 (2005), a case involving a medical necessity for the use of marijuana, opined during oral arguments that “medicine by regulation is better than medicine by referendum.” The Court’s 6-3 decision, which Justice Breyer joined, upheld the prohibition of marijuana for medical use under the Controlled Substances Act (CSA). The FDA’s novel standard in recommending marijuana’s rescheduling is rooted in a logical fallacy: some people say that marijuana is medicine, so marijuana must be medicine. The FDA is delegating its authority to determine that medications are safe and effective to popular opinion, a practice that not only exceeds the statutory authority of the agency but makes a mockery of the congressional intent of the Food, Drug, and Cosmetic Act to protect the public health. Following the FDA’s logic, psychedelic drugs, which are seeing a popular push for medical legalization, could also be considered medicine and be rescheduled due to shifting public opinion.
4. The FDA compares marijuana to a limited, hand-picked list of other controlled and noncontrolled substances (e.g., heroin, alcohol, cocaine), not all Schedule I drugs.
In the recommendation, the FDA measured marijuana’s potential for abuse by comparing it to a hand-picked selection of Schedule I, II, and III drugs. For example, the FDA compared marijuana to heroin, another Schedule I drug. The recommendation claims that because marijuana has a lower abuse potential than heroin, it shouldn’t be in the same category. Yet the FDA failed to compare marijuana to other Schedule I drugs, such as LSD. Comparing marijuana’s abuse potential against all Schedule I drugs would have allowed for a more rigorous analysis, but it would not have allowed the FDA to conclude that marijuana belongs in Schedule III. To qualify for Schedule III, a drug or other substance must have “potential for abuse less than the drugs or other substances in Schedules I and II” (21 USC 812(b)). Fifty years of data published by HHS show that marijuana does not meet this standard.
5. None of the studies used by the FDA to justify its claim that marijuana is medicine support that conclusion.
The FDA determined that marijuana is acceptable for medical use for pain, nausea and vomiting, and anorexia. Only three studies were used to justify this claim. The first (University of Florida), concluded that results were “inconclusive or mixed.” The second (National Academies of Sciences & Medicine) relied primarily on a study for which the results were not statistically significant. For the third (Agency for Healthcare Research and Quality), the FDA concluded that the positive effects of marijuana in the study were small and that “the increased risk of dizziness, nausea, and sedation [from marijuana use] may limit the benefit” (page 27 of 252). Furthermore, some of these studies were with inhalable marijuana; prior FDA evaluations have excluded inhalable marijuana studies because of their unreliability and questionable practices.
You Can Be Addicted to Weed. I Was When I Was 12.→
/
Boomers who fought for legalization have no idea how dangerous it is.
Read MoreBrutal Marijuana Studies Now Emerging - It Should Never Have Been Fully Legalized
/
For years, marijuana advocates claimed that if only America would loosen restrictions, we'd all see how beneficial the drug is. But now, more than 10 years after the first efforts to do just that, we are seeing that the critics were right. Liberal pot laws and increased usage are far from the panacea pot-lovers claimed. Starting back in 2012, Colorado passed a law to allow private use of marijuana. Soon the state of Washington joined the Centennial State in loosening its pot laws. And many more came in the following years, especially when the states began to realize it could tax "legal" marijuana and bring millions into their state treasuries. Now even the federal government is looking to loosen the reins and is preparing to take pot off its Schedule One prohibitions, a move said to be the first step in decriminalizing marijuana. But now these states are finding that it is time to pay the piper, as a raft of ill-effects are spreading like wildfire all across the country. From mental illness to addiction and impaired driving, the effects on many are not as beneficial as advocates claimed. There do seem to be a very few beneficial uses for pot for a small number of people. It does help in pain relief for the chronically afflicted, it can help with nausea from chemotherapies and it is sometimes effective for those with anxiety. But all those benefits are limited and are far outweighed by the deleterious effects seen when widespread use is factored in, according to a raft of new studies reported by the Daily Mail. With a pool of more than 40 million pot users to look at, researchers are finding that recreational use of the drug is becoming an increasing problem everywhere it is being tried. As the Mail noted, researchers from the Aarhus University Hospital in Denmark have found that despite claims by pot advocates, the drug is just as addictive as any other drug. And 41 percent of users have developed major problems with depression. The research found that chronic marijuana use quadrupled risk of developing a bipolar disorder and added to a rise in psychotic breaks, including thoughts of, and deaths by, suicide, with pot linked to 30 percent of cases of schizophrenia. The researchers added that people who already have a propensity for these mental disorders often find that pot makes them worse, not better. That is nothing like the benign effects pot advocates claimed we'd be seeing. Pot advocates also claimed that one can't really become addicted to the drug. This has also been revealed as false. "New research from University of Washington and Kaiser Permanente Washington Health Research Institute estimates 21 percent of marijuana users had become addicted," the Mail reported, adding that at least four million Americans have developed "marijuana use disorder" since pot became so much easier to get. Another claim that many advocates have made is that pot will calm you and make sleep come easier. This is also not true, studies have found. "A 2021 study in the journal BMJ reported adults who used cannabis 20 or more times in the previous month were more likely than non-users to get six or fewer hours of sleep per night," the Mail reported. In addition, 39 percent of daily pot users developed clinical insomnia. An even more alarming study says that pregnant women will put themselves at a 70 percent higher risk of birth defects if they regularly use pot during pregnancy, and they will be 2.3 times more susceptible to a stillbirth. Also, "A 2022 study published in JAMA Pediatrics found prenatal cannabis exposure after five to six weeks of pregnancy is associated with attention, social and behavioral problems that persist into early adolescence," the Mail reported. Finally, the evidence seems irrefutable that heavy pot smoking is just as bad on your body as heavy tobacco smoking. Smoking anything -- pot or tobacco -- increases the risk of coronary artery disease and also puts users at an increased risk of lung disease. A study from Canada found that "three-quarters of marijuana users had emphysema - a lung disease which leaves sufferers struggling to breathe -- compared to two-thirds of tobacco users," the Mail wrote. While it might be a better idea to go to a prescription model, where only seriously ill people are able to gain access to pot, it seems clear that recreational and non-medicinal use has had detrimental effects on Americans.
How Do You Know if You’re Addicted to Weed?→
/
Nearly 6 percent of American teens and adults have cannabis use disorder.
Read MoreAre state fair officials high? They should not reward super-potent marijuana→
/
Cannabis is making its debut at the California State Fair in July, taking its place among chardonnays, craft brews, tomato salsas, pickled peppers and satsuma marmalades as a product of the state’s agricultural bounty.
Read MoreCopycat pot edibles that look like candy are poisoning kids, doctors say→
/
Dr. Jane Pegg couldn't believe her eyes when she saw the pot edibles that had poisoned a two-year-old who had been rushed to the emergency room in October.
"It so shocked and appalled me … the package looked almost identical to gummies that are sold as candies in the store," the Nanaimo, B.C., pediatrician said.
Read MoreAnother sad story of loss brought to us by the marijuana industry.
/By Aubree Adams
I absolutely loved living in Colorado.
Family-oriented Pueblo is the state’s best-kept secret. Lake Pueblo, Pueblo Mountain Park, and Devil’s Canyon are perfect places to hike. We lived in an old Craftsman home in the historic district, with a beautiful garden and wonderful neighbors. I felt like I was living in a dream.
And then legalized marijuana came, and everything changed. It’s taken nearly a decade for Colorado’s elected leaders to understand the damage pot is doing to our children. I saw it years ago.
My eldest son entered eighth grade in 2014, the year recreational marijuana stores opened in Colorado. Soon, his behavior changed. He became irrational and repeated things that didn’t make sense. I dismissed it as adolescent mood swings. He’d just broken up with a girlfriend. That’s all it was, I told myself.
By his freshman year, I realized he was using marijuana. I was still in denial, though, until he attacked his younger brother and then tried to kill himself. The hospital treated him and sent him home. A few days later, when it was clear he was still suicidal, I took him back to the emergency room. Don’t worry, they told me. It’s just marijuana.
Marijuana is a serious drug
Eventually, my son told me he was dabbing, which I had never heard of. A dab (or wax or shatter) is a highly concentrated form of THC, marijuana’s active ingredient. It’s heated and smoked, delivering an instant, overwhelming high. Crack weed, my son called it. He knew it was making him crazy. He wanted to quit, but addiction had him firmly in its grip.
And yes, he was addicted. Addiction is a pediatric disease. In 9 out of 10 cases, it originates with drug or alcohol use before age 21. Marijuana, which has been linked to mental illness and psychosis in teens and young adults, slowly takes away your humanity. That’s what it did to my son, who turned to running the streets with homeless people. He had no trouble finding people to feed his addiction in return for selling their legally home-grown marijuana.
I quit working, making it my full-time job to save my son. I soon found out that getting treatment wasn’t easy. Beds were full. Officials minimized marijuana's addictiveness.
I found a highly regarded treatment center in Utah; they required $36,000 up front that I didn't have. Finally, I found a place in San Diego that helped restore his health. He regained confidence and looked good. In the meantime, I had learned about a recovery community in Houston, where host families provide positive peer support. My son got better when he left Colorado, so I moved him there in 2016. My other son, who had developed post-traumatic stress disorder, and I followed in 2018.
Rein in this monster
Sadly, my story isn’t unique. Families across Colorado have experienced the same heartbreak and worse. More and more, marijuana is implicated in teen suicides. From 2014 to 2018, marijuana was present in nearly one-third of teen suicides. Pot is taking our children from us.
That’s why a bipartisan legislature this year passed a bill that begins to rein in this monster. The bill:
► Authorizes a study on the effects of high-potency THC products on the developing brain and how to keep those products away from teens. These unbiased experts will make a recommendation for next steps to the legislature.
► Requires doctors issuing medical marijuana recommendations to consider the person's mental health history;
► Orders a report on hospital discharge data when marijuana use is likely;
► Directs coroners to screen for THC in non-natural deaths;
► Reduces the amount an 18-year-old medical card user can purchase in a single day. This closes a loophole that could be exploited to stock up on marijuana concentrates, which they sell to their younger friends.
It’s a baby step, but it’s significant that the state that pioneered marijuana legalization is finally recognizing there are harmful consequences.
We can’t keep going down this road. We can’t keep sacrificing our children on the altar of pot. Big Marijuana promotes high-potency, addictive concentrates with no proof they are safe for anyone. Colorado’s commission, when it reviews all the research already done, will confirm that this product is dangerous to children and much too easy for them to get.
Maybe lives will be saved. Maybe other states will be warned against following Colorado’s lead Maybe no more families will have to endure the hell that mine has.
But it comes too late for me and my oldest son. He started using again. I haven’t seen him in a year.
Aubree Adams is director of Every Brain Matters. She is the parent coordinator for a Houston recovery community, where she lives with her youngest son and two dogs.
Are scientists missing the forest for the trees on youth marijuana use?→
/
Are scientists missing the forest for the trees?
Last week, the Journal of the American Medical Association published a study by DM Anderson and colleagues, scientists from universities in Montana, Spain, and San Diego, California. The study finds that legalization does not increase adolescent marijuana use. The researchers analyzed the Youth Risk Behavior Surveillance System (YRBSS) which the Centers for Disease Control and Prevention (CDC) began conducting in 1991.
Youth Risk Behavior Surveillance System (YRBSS)
YRBSS collects data from high school students every two years about behaviors that contribute to unintentional injuries and violence, sexual behaviors related to unintended pregnancy and sexually transmitted infections, alcohol and other drug use, tobacco use, unhealthy dietary behaviors, and inadequate physical activity. Not all states participate in YRBSS, and those that do participate periodically, although in the 2019 YRBSS all but five states did so. Minnesota, Oregon, and Washington State have never participated in YRBSS. The survey asks three questions about marijuana: ever use, current use, and what age students were when they started using marijuana. It began asking about vapor product use in 2015, but never asks what students are vaping.
So far as these limited data are concerned, the researchers’ findings seem true. But two other national surveys show us something more.
The National Survey on Drug Abuse/National Survey on Drug Use and Health
The National Survey on Drug Abuse is the oldest. It began in 1971 and was financed by the National Institute on Drug Abuse (NIDA). Its first two surveys were done under the auspices of the National Commission on Marihuana and Drug Abuse. It began publishing annual data in 1976 and was transferred to the newly created Substance Abuse and Mental Health Services Administration (SAMHSA) in 1992. Technological innovations enabled the survey to be redesigned in 1999 and its name was changed to the National Survey on Drug Use and Health (NSDUH) in 2002. However, the redesign of the renamed survey resulted in an inability to compare its results with findings from the National Household Survey on Drug Abuse.
The NSDUH collects data annually on the use of alcohol, tobacco, marijuana, and other drugs from adolescents (ages 12-17), young adults (ages 18-25), and older adults (ages 26 and older). It combines two years of data to report drug use among these age groups by state but unfortunately not before 2002. RTI is the contractor responsible for administering this survey, which also collect data on the mental health of Americans.
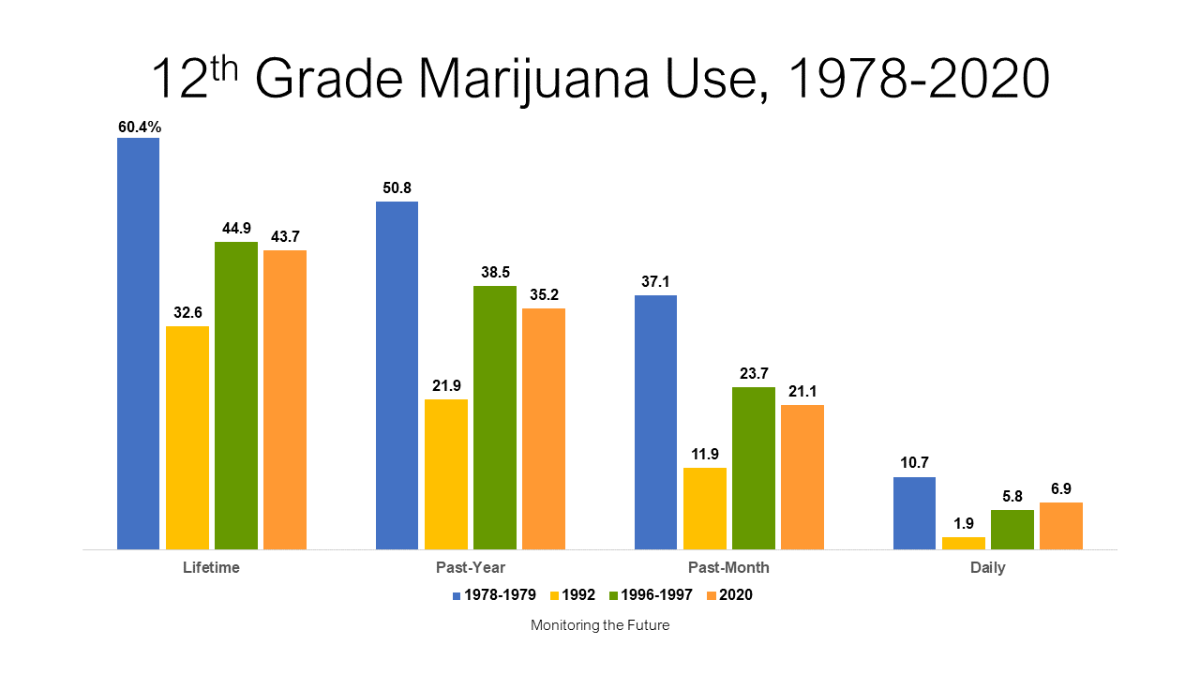
Monitoring the Future (MTF)
The third national survey is Monitoring the Future (MTF), which began in 1975. Financed by NIDA, MTF is the only survey that can give us continuous data from 1976 through today. It collects data about the lifetime, past-year, past-month, and daily use of alcohol, tobacco, marijuana, and other drug by students in grade 12. It added students in grades 8 and 10 in 1990. In 2015, MTF began asking about vaping and two years later asked specifically what kids were vaping – nicotine, marijuana, or just flavoring. Unfortunately, it does not report its data by state. The University of Michigan Institute for Social Research administers this survey.
The chart above shows that drug use among high school seniors peaked in 1978-1979. A 1977 study called Highlights from the National Survey on Drug Abuse estimates that in 1962, less than 2 percent of the US population and less than 1 percent of adolescents had ever tried an illicit drug. Over the next 16 years, “ever-tried” use rose among seniors to 60.4 percent, while 50.8 percent of seniors used the drug in the past year, 37.1 percent used it in the past month, and 10.7 percent used it daily. What drove that astonishing escalation in use among 18-year-olds?
Decriminalization and Drug Paraphernalia
The National Organization for the Reform of Marijuana Laws (NORML) formed in the early 70s and initiated a movement to decriminalize marijuana. Decriminalization then was defined as reducing criminal penalties for possessing an ounce or less of marijuana, enough for personal use. In 1973, NORML persuaded Oregon to decriminalize marijuana and in rapid succession over the next five years,10 more states decriminalized. By 1978, eleven states had reduced marijuana penalties to that of a traffic ticket. Along with decriminalization emerged the drug paraphernalia industry called by some “little learning centers for young drug abusers.” Head shops (shops for “heads” as the industry called drug users) selling child-appealing toys and gadgets to enhance drug use opened in urban and suburban communities across the US throughout the 70s, leaving no doubt in parents’ minds that a drug paraphernalia industry was coming after their kids. Studies showed that children reasoned a government would not reduce penalties for a drug that could hurt them.
The Parent Movement
This gave rise to a national Parent Movement which began in Atlanta in 1976 and spread across the nation. The movement was based on three goals: join with other parents to protect kids from becoming drug users, shut down headshops, and stop decriminalization. Some 3,000 parent groups from the mid-70s to the early 90s formed parent peer groups to protect their children and their children’s friends from using drugs. Many, usually in state capitals, became politically active. Their efforts to persuade legislators to pass laws outlawing drug paraphernalia drove the industry out of business. No more states decriminalized marijuana over the next several decades. NORML’s funding nosedived forcing the organization to severely curtail its decriminalization crusade.
Between 1978-79 and 1992, high school seniors’ marijuana use plummeted:
Lifetime use was cut nearly in half from 60.4 percent to 32.6 percent.
Past-year use dropped by more than half from 50.8 percent to 21.9 percent.
There was a three-fold decrease in past-month use, and a
five-fold decrease in daily marijuana use.
The first two directors of the National Institute on Drug Abuse, Robert DuPont, MD, and William Pollin, MD, credit the Parent Movement with bringing about this significant reduction in marijuana use among adolescents. But in just four years, these gains reversed:
Seniors’ lifetime marijuana use rose from 32.6 percent in 1992 to 44.8 percent in 1996-1997.
Their past-year use nearly doubled over those four years, from 21.9 percent to 38.5 percent.
Past-month use among seniors did double, and
Daily use rose more than three-fold.
What made that happen?
Medical Marijuana
In 1992, three billionaires began pumping money into a by-then moribund NORML as well as into two new groups, the Marijuana Policy Project, and a coalition of other groups that became the Drug Policy Foundation. They targeted states that allow ballot initiatives, made unsubstantiated claims about the healing powers of marijuana, bought voters’ signatures, and placed measures to legalize marijuana as medicine on the ballots of states few lived in, leaving taxpayers to pay for the consequences of their actions. A steady stream of media stories across the nation educated children that pot is medicine and they responded in kind. If a government wouldn’t reduce penalties for a drug that could hurt you, that drug surely couldn’t hurt you if it was medicine! The national cacophony that led up to the first state legalizing pot as medicine – California in November 1996 – carried that message and kids heard it loud and clear.
The National Household Survey on Drug Abuse shows much of these same patterns for both adolescents and young adults during the 70s, 80s, and 90s. But since that survey’s data cannot be compared to NSDUH’s, the best we can do is look at the most recent survey, which is the 2018-2019 state estimates. The following two charts are created on the same vertical axis of 0 percent to 60 percent. The first one shows past-year marijuana use among adolescents, the second among young adults.

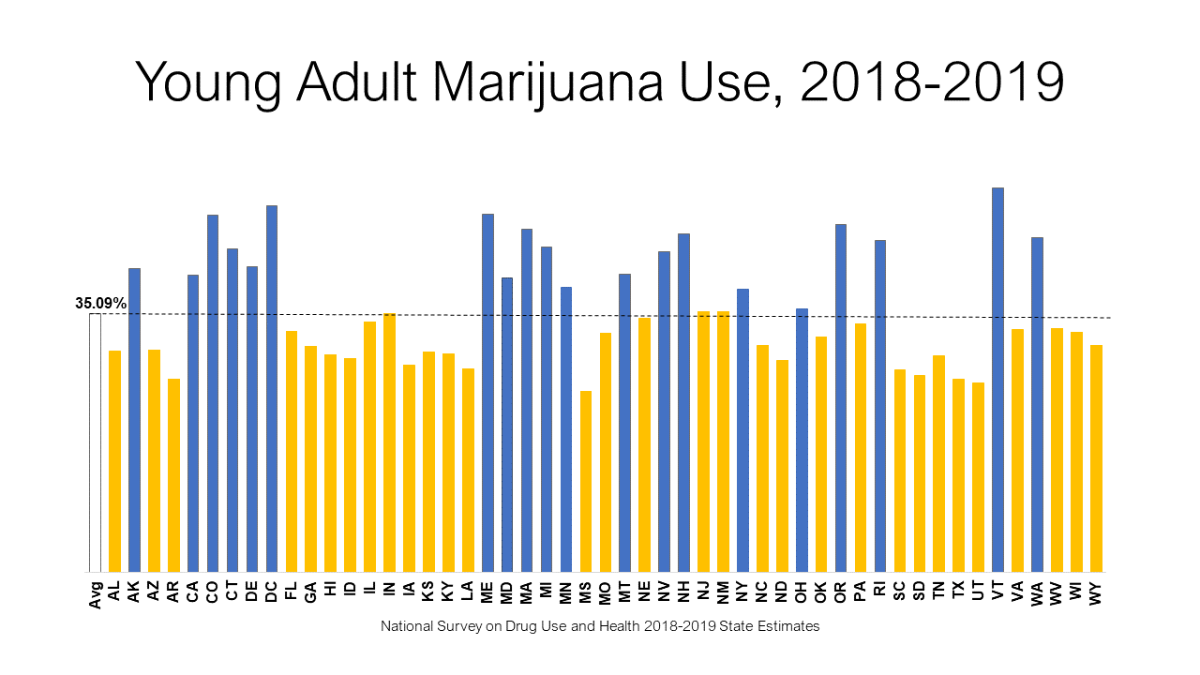
No, not all of the blue bars are recreational states and yes, some of the yellow bars are. But 36 of these states have legalized marijuana for medical use and that has influenced young people ages 12 to 25 to engage in its use. Like decriminalization in the 70s, the novelty of turning pot into medicine with an intensive four-year campaign championed by national media has not only had a profound effect on the nation’s young people but also introduced a unique way to approve medicines by ballot-iinitiative and, later, legislative fiat rather than through the Food and Drug Administration. Should we worry that advocates are now applying that pattern to other drugs?
Access these graphics here.
Access YRBSS here.
Access NSDUH here.
Access MTF here.
Read National Survey on Drug Use and Health: Summary of Methodological Studies, 1971-2014 [Internet] here.
Medical cannabis unlikely to benefit most chronic pain patients, international researchers say→
/
“So medical cannabis is not likely to be a panacea. It is not likely to work for the majority of individuals who live with chronic pain. We do have evidence that it does appear to provide important benefits for a minority of individuals,” said Busse, who is also a chiropractic doctor.
Read MoreAre Marijuana Use and Suicide Linked? — A review of the data show there's cause for alarm→
/
Data linking marijuana use to people with suicidal ideation, attempts, and completed suicides are steadily increasing.
Read MoreThe True Cost of Marijuana: A Colorado Town That Went All-In→
/
Emergency room doctors in Pueblo see a different side of the equation and say the deleterious effects of cannabis legalization far outstrip any benefits.
Read MorePoliticians must recognize Americans' changing perceptions of marijuana→
/
It was no surprise then that our survey found two-thirds of Americans support curbs on the commercialization of marijuana, and 78 percent want to see warning labels (similar to those on alcohol and tobacco) on pot products.
Read MoreMarijuana Is Not a Public Health Solution to the Opioid Crisis→
/
Making marijuana more available might appear to be a solution to the current drug crisis in our nation. However, a more critical look at the research evidence suggests just the opposite. Decades of research findings have shown that marijuana use puts an individual at heightened risk for misuse of prescription opioids, heroin and other drugs.
Read MoreCash from cannabis companies creates conflicted researchers→
/
Universities in both Canada and the United States have recently accepted multi-million-dollar donations from the cannabis industry.
Read MoreThese California politicians once helped regulate legal marijuana. Now they’re working for the industry→
/
The pot industry hiring ex-officials is particularly egregious because of the harm this industry does to kids, young adults, families, communities and the country in general
Read MoreExpanding legal access to marijuana is not the solution to America's opioid crisis
/
Expanding legal access to marijuana is not the solution to America's opioid crisis, according to a new research analysis published by the nonprofit Hazelden Betty Ford Foundation.
Read MoreLegalizing pot is proving to be a public-health disaster→
/
It’s becoming increasingly obvious that legalizing marijuana consumption was a colossal public-health blunder.
Read More